"Weird Al" Yankovic returns with an awesome parody of Blurred Lines. The American language has devolved into text-speak and emojis. Weird Al takes on every complaint about language in this video that will probably show up in every English class across the country. I mean ... these grammer mistakes literally makes my head explode and I definitely LOLed at it's message.
Enjoy!
Friday, July 25, 2014
Thursday, July 24, 2014
Be A Man
 While I coached high school football, the school board became attached to a 1970's football player turned coach and pastor, Joe Ehrmann. His son played for Wake Forest and since he was around a lot, he would come and speak to us ... a lot. He spoke at a Faculty Meeting, School Coaches Meeting, County Coaches Meeting, and a Youth Camp. Every coach in the county was given the book Season of Life, by Jeffrey Marx about Ehrmann's successes as player and coach of Gilman High School. Recently, Joe sat down with NPR's All Things Considered to talk about what it means to be a man.
While I coached high school football, the school board became attached to a 1970's football player turned coach and pastor, Joe Ehrmann. His son played for Wake Forest and since he was around a lot, he would come and speak to us ... a lot. He spoke at a Faculty Meeting, School Coaches Meeting, County Coaches Meeting, and a Youth Camp. Every coach in the county was given the book Season of Life, by Jeffrey Marx about Ehrmann's successes as player and coach of Gilman High School. Recently, Joe sat down with NPR's All Things Considered to talk about what it means to be a man.Coaches have an enormous power to mold young men, and women, through their high school career. During those four years, a scrawny 14-year-old boy develops into an 18-year-old man about to head out into the world. No doubt that at some point, every male has heard the phrase, "Be a Man". But mostly, no one ever explains what that means. Joe Ehrmann believes that the old view of masculinity revolved around three basic lies - Athletic Ability, Sexual Conquest and Economic Success. Your manliness is essentially on a scale based on these three attributes. Instead, Joe argues, manhood should be about your capacity to love and your commitment to a cause. We should be building relationships instead of walls.
Joe Ehrmann gives a great talk and I urge to to listen to the NPR link or to check out the book.
Wednesday, July 23, 2014
H-IPPE: Clinical Generalist
 |
| Clinical generalists work on the floor within the medical team |
Because I was on the evening shift, there really wasn't much to see other than order verification. She went incredibly fast clicking away as they came in. Several warnings would pop up on orders that she would override. She explained that our clinical judgement allows us to get past some warnings when the benefits outweigh the risks. Some medications are hazardous with serious potential complications, but if it cures an infection quickly, it would be worth it. A few times, the clinical generalist calculated Creatinine Clearance (CrCl) to determine a patient's kidney function which would result in an adjustment of the dosage. Had I seen a day shift, my experience would have included rounding with the medical team as the generalist makes dosage suggestions.
Usually, a clinical generalist completed one year of residency training. I enjoyed the experience and would not mind falling into that type of position. While I may not know all the clinical information yet, you do seem to work towards the peak of your certification making judgement calls and having a potentially active role in patient care on the floor. Nurses would stop by and ask questions or we would search out doctors to make suggestions. Most importantly, the clinical generalist on the floor helps catch medication errors and optimize patient care.
Tuesday, July 22, 2014
TED Talk Tuesday: Ric Elias
Ric Elias was a passenger on the fateful flight that left NYC only to be landed in the Hudson River. He talks to TED with the clarity that can only be revealed when the pilot comes over the intercom and says, "Brace for impact".
Enjoy!
Enjoy!
Monday, July 21, 2014
H-IPPE: Central Outpatient Pharmacy

Many of the pharmacists previously worked at CVS or other retailers before coming to the COP. That was part of the manager's plan to decrease the wait times for the patients. Apparently a year ago, patients waited for an hour, while now they are in and out in 20 minutes. The pharmacist that I spoke to was really happy with his choice to leave retail and come to the COP. There may have been a major pay cut, but greater quality of life - including less weekends and an actual lunch hour. It is a lot easier to help the patients because they are attached to the hospital network and can view the entire hospital record for a patient and determine the indication. Knowing the indication can help with verifying a medication's dosage, especially for pediatrics. For all pediatric prescriptions, they must recalculate the dosage strength. This requires the child's weight in kilograms and the indication - both readily available in the COP, not at a local retailer.
As a public hospital devoted to all North Carolina residents, the COP has a pharmacy assistance program for those that cannot pay. Some have $4 copays or even zero. Many patients come from 2-4 hours away to receive their heavily discounted drugs, which is why the hospital is pioneering a mail order program. Before a patient qualifies for the assistance program, the COP will fill any order for 14 days. When they come back with the forms and are accepted they will fill the remainder of the order.
Even though I may not know what I want to do in the end of the PharmD program, this was one that I definitely felt comfortable with. I hear the stories about working in retail and the difficulty of getting into a clinical position, but this sits firmly in the middle. You help patients on their transition from the hospital to home and you get to use more of your clinical knowledge to help. I would have no problem working in an outpatient pharmacy after this experience.
Friday, July 18, 2014
Be a Good One
If you are going to do something, be the best at it. Doesn't matter what it is, try your hardest. You may not become the best, but you will get better. You will find where your talent lies and potentially impress the right people to get you where you want to be.
This is Rule #2
This is Rule #2
Wednesday, July 16, 2014
HIPPE: Carolina Care at Home
 Of my three days with the Med Transition Specialists, I spent one day with another subset of the group called Carolina Care at Home (CC@H). While med histories dealt with people through the admission into the hospital, this group works with the discharge of patients. Essentially, CC@H extends the Central Outpatient pharmacy into a bedside delivery service before patients leave the hospital. There are benefits for both parties. The patient doesn't have to stop at a local pharmacy on the way home to pick up prescriptions, and the hospital generates revenue from the sales.
Of my three days with the Med Transition Specialists, I spent one day with another subset of the group called Carolina Care at Home (CC@H). While med histories dealt with people through the admission into the hospital, this group works with the discharge of patients. Essentially, CC@H extends the Central Outpatient pharmacy into a bedside delivery service before patients leave the hospital. There are benefits for both parties. The patient doesn't have to stop at a local pharmacy on the way home to pick up prescriptions, and the hospital generates revenue from the sales.We started early in the morning by checking the eligibility of the patients about to be discharged from the hospital. Because there are only four members of this group, they focus on patients with insurance instead of self-pay. After identifying potential customers, we went through the floors to offer them the service. After watching the person I was shadowing a few times, I felt comfortable enough to give it a go. I walked into a patient's room a little nervous, but prepared. The 26-year-old patient was alone in his room watching TV when we entered. I asked if he would be interested in bedside delivery, but I didn't get much feedback from him. I kind of freaked out that I was bad at this and every patient would respond to me in the same way. After leaving, a nurse let us know that he had the mental capacity of a 5-year-old and probably didn't understand what we were saying. When we spoke to his guardian later that morning, I noticed that the patient was watching Sesame Street on the TV. Fortunately, not all of the patient encounters turned out that way. In fact, pretty much everyone I spoke to was eager to have the meds delivered before leaving the hospital - except one patient that received free medications on the military base. Of any day on the HIPPE rotation, I spoke to the most patients with the CC@H.
After a patient agreed to CC@H, we would fax their prescriptions down to the Central Outpatient Pharmacy and let them know something was coming. The popular service could easily overwhelm the staff down there in their little corner of the COP, so it would not be surprising for a 2 hour turn around. When we went through the floors of her service area, we headed down to the COP to pick up the orders and take them back up to the rooms. After we left, a pharmacist in the COP would call the patient's room, counsel them on the medications, and collect their payment over credit card. If the patient paid in cash, we brought up the meds, took their money to the pharmacy, and brought their change back up to the room. There was a lot of walking done on this day. Actually, because I have a FitBit I can tell exactly how much walking was done - 14,000 steps for over 5 miles. For this job, comfortable shoes are a must.
Overall, the Carolina Care at Home initiative is a great program. The pharmacy can reach out to a hospital full of confined customers. Patients can receive what they need before leaving and head straight home. I don't know if other hospitals have a similar program, but if I end up in one that doesn't I will attempt to start it. Transitions of care is a hot topic in the health care field. This can earn money from the hospital and help prevent patients from readmission. Win-Win.
H-IPPE: Transitions of Care
Spurred by the Affordable Care Act, hospitals have turned their focus to reducing hospital readmission rates. Medicare will no longer reimburse hospitals if a patient is readmitted to the hospital within a month of their discharge. To prevent these readmissions, hospitals take great interest in the transitions of care - admission, transfers, and discharges - for at-risk patients. High-risk patients are determined by
age, comorbidities, multiple medications, and economic status. Once a patient is identified, the Med Transition Specialists come into play to collect a complete and accurate Medication History. On this team, we spent three days during our rotation. Though all the IPPE's had different experiences, I enjoyed my time interacting with patients and feeling like I had an impact on their admission to the hospital.
Medication histories are generally taken by the nurses when a patient has been admitted. A lot of the time, the nurse can just copy and paste from their medical records. But time and again, this has shown to lead to inaccuracies and missed medications. Nurses have huge responsibilites in caring for the patient, the pharmacy department is best suited to taking care of a patient's medications. So at UNC and other hospitals, a team of pharmacy technicians review the collected histories which a pharmacist checks off for medication errors or duplications of therapy.
Unfortunately, the Med history team at UNC only consists of four technicians for the entire hospital. The means that they must focus on the high or moderate risk patients when collecting patient histories. The process was relatively simple.
In the end, I found the people interesting and enjoyed working on real patients. Med Histories are important to provide the doctor with a full background of the patient before coming into the hospital. Later during the month, I wound up on pediatric rounds for patients if cystic fibrosis. The medical team had a long debate about what the kid was taking at home and how much we should give them while in the hospital. Since Med Transitions only have 4 technicians, they can't get everywhere. Perhaps the automation of the pharmacies will open up technicians to move to roles of taking med histories through out the hospital. I know that the focus is on high-risk medicare patients, but all patients are at some risk when they transition from one place to another. And pharmacists are the best suited members of the medical team to oversee those transitions.
 |
| This patient is high-risk for readmission and needs medication review and reconciliation. |
Medication histories are generally taken by the nurses when a patient has been admitted. A lot of the time, the nurse can just copy and paste from their medical records. But time and again, this has shown to lead to inaccuracies and missed medications. Nurses have huge responsibilites in caring for the patient, the pharmacy department is best suited to taking care of a patient's medications. So at UNC and other hospitals, a team of pharmacy technicians review the collected histories which a pharmacist checks off for medication errors or duplications of therapy.
Unfortunately, the Med history team at UNC only consists of four technicians for the entire hospital. The means that they must focus on the high or moderate risk patients when collecting patient histories. The process was relatively simple.
- Print off the Medications Prior to Admissions from EPIC (computer system)
- Call the pharmacy if listed in their records to get their last refills (dates and quantities)
- Interview the patient to confirm which medications their are taking (and how)
- Make notes in EPIC regarding med use in records.
In the end, I found the people interesting and enjoyed working on real patients. Med Histories are important to provide the doctor with a full background of the patient before coming into the hospital. Later during the month, I wound up on pediatric rounds for patients if cystic fibrosis. The medical team had a long debate about what the kid was taking at home and how much we should give them while in the hospital. Since Med Transitions only have 4 technicians, they can't get everywhere. Perhaps the automation of the pharmacies will open up technicians to move to roles of taking med histories through out the hospital. I know that the focus is on high-risk medicare patients, but all patients are at some risk when they transition from one place to another. And pharmacists are the best suited members of the medical team to oversee those transitions.
Tuesday, July 15, 2014
TED Talk Tuesday: Keith Barry
Keith Barry describes himself as a mentalist. He steps onto the TED stage to perform some brain magic in one of my favorite videos of all time. Magic is mastery of the human brain, and Keith Barry is a grand master. I showed this one to every class, mostly to get them interested in TED.
After showing this in class, I learned some of the techniques. I tried teaching this kids how to read someone's mind and here is one to try. Have a partner pick a number 1 to 20. Start counting from one and carefully watch their pupils. While there face may not react when you get to the number, their pupils will never lie. When you see them change, that should be the number. The change is subtle and it clearly takes years of practice to master. Notice that Keith performs the feat with letters to determine the ex-boyfriend's name. Small reactions and experienced guessing gets him to the right answer.
Enjoy and see if you can figure out the Coke bottle trick!
After showing this in class, I learned some of the techniques. I tried teaching this kids how to read someone's mind and here is one to try. Have a partner pick a number 1 to 20. Start counting from one and carefully watch their pupils. While there face may not react when you get to the number, their pupils will never lie. When you see them change, that should be the number. The change is subtle and it clearly takes years of practice to master. Notice that Keith performs the feat with letters to determine the ex-boyfriend's name. Small reactions and experienced guessing gets him to the right answer.
Enjoy and see if you can figure out the Coke bottle trick!
Monday, July 14, 2014
H-IPPE: Investigational Drug Service
For my first rotation for the month of May, I visited one of the different departments at the hospital. The Investigational Drug Service (IDS) controls the distribution of all drugs related to clinical trials taking place throughout the hospital. Not every hospital runs 200-400 clinical trials at the same time and often lack an IDS department. The investigational drug service dispenses every drug related to clinical trials with the UNC system, including the hospital, Medicine, Dentistry, Pharmacy, Public Health, etc. The drugs include some commercial products being tested for other indications, but also drugs from companies with just letter-number designations. The third floor office takes care of the IV preparations of drugs. We had Zithromax for C-section s and a few others. They have to be very careful about storing the medications and keep detailed records about the temperatures of the refrigerator. While I was there the electrician changed over the circuits for the wing, which shut down the refrigerators for 10-15 minutes. They eyed the thermometers as the temperature approached 8 degrees C - the point that they would have to fill out special forms for each and every one of the drugs in the refrigerator.
My favorite part of the department is the use of placebos. In more modern clinical trials, the traditional placebo is used less frequently. If a new drug needs to be tested, it must be compared to the current, accepted standard method of treatment. So the "placebo" group will receive the standard treatment, and the experimental group will receive both the standard treatment and the added treatment to be investigated. In most cases, a protocol exists and the new drug seeks to improve upon it. These standards change with new drugs every year. For instance, if Sovaldi becomes the standard treatment every ongoing clinical trial comparing the old protocol will become invalid. Most modern placebo experiments involve adding a drug to the current treatment. If a disease is treated with A+B, a clinical trial may determine if A+B+C works better. Double-blinding begins at the IDS office. In most trials, they enter the patient into a computer database that randomly assigns them to the new drug or placebo. In some trials, even the pharmacist does not know which group the patient belongs to. Other trials are "open label" and will indicated exactly what the treatment is on the drug label itself and all parties will know exactly what treatment is being administered. This method is implemented in trials that use a standard of care as a base treatment.
To protect the doctors and nurses doing the trials for themselves or for big pharmaceutical companies, the IDS controls the blinding process by randomly assigning the new drug or the placebo to the patient. Often, only the pharmacists and technicians in IDS know whether they have given the drug or placebo. When an order comes in, the request is put into a computer system that spits out the result of an algorithm to determine what the patient should receive. Sometimes, the nurses are accidentally unblinded through the process. In one instance, the trial was to determine the appropriate strength of drug - 10mg/mL vs 15 mg/mL. However, the new computer system requires a strength to print the label to dispense the medication. As soon as 15 mg/mL shows up on the label, everyone knows what group the patient belongs to - thus unblinding trial. When I left for the month, they were attempting to enter zeros for the concentration. I never learned of the resolution.
My favorite part of the department is the use of placebos. In more modern clinical trials, the traditional placebo is used less frequently. If a new drug needs to be tested, it must be compared to the current, accepted standard method of treatment. So the "placebo" group will receive the standard treatment, and the experimental group will receive both the standard treatment and the added treatment to be investigated. In most cases, a protocol exists and the new drug seeks to improve upon it. These standards change with new drugs every year. For instance, if Sovaldi becomes the standard treatment every ongoing clinical trial comparing the old protocol will become invalid. Most modern placebo experiments involve adding a drug to the current treatment. If a disease is treated with A+B, a clinical trial may determine if A+B+C works better. Double-blinding begins at the IDS office. In most trials, they enter the patient into a computer database that randomly assigns them to the new drug or placebo. In some trials, even the pharmacist does not know which group the patient belongs to. Other trials are "open label" and will indicated exactly what the treatment is on the drug label itself and all parties will know exactly what treatment is being administered. This method is implemented in trials that use a standard of care as a base treatment.
To protect the doctors and nurses doing the trials for themselves or for big pharmaceutical companies, the IDS controls the blinding process by randomly assigning the new drug or the placebo to the patient. Often, only the pharmacists and technicians in IDS know whether they have given the drug or placebo. When an order comes in, the request is put into a computer system that spits out the result of an algorithm to determine what the patient should receive. Sometimes, the nurses are accidentally unblinded through the process. In one instance, the trial was to determine the appropriate strength of drug - 10mg/mL vs 15 mg/mL. However, the new computer system requires a strength to print the label to dispense the medication. As soon as 15 mg/mL shows up on the label, everyone knows what group the patient belongs to - thus unblinding trial. When I left for the month, they were attempting to enter zeros for the concentration. I never learned of the resolution.
The IDS could be a really
interesting area, at the forefront of future medicine. There is a ton of
paper work with monitors coming every so often from the companies to make sure
everything is documented correctly. But they could be dispensing the
trial drugs that are the next wave of pharmacy. They performed several
sofosbuvir trials that have have a lot of HIV and HCV researchers and
clinicians excited. If you appreciate the scientific method with blinds,
placebos, and protocols, you would enjoy the IDS.
Friday, July 11, 2014
Lucky Fish

Thursday, July 10, 2014
The Broken Escalator
Do you ever have some place to go, but then get stuck on the path. Maybe you are in school for a specific target, but don't feel that the teachers or professors are helping you get there. Do you complain and wait for them to help you? Or do you take matters into you own hands? Education is not dispensed from on high, but a journey to explore one step at a time. Pay attention in class, but also read the book, ask questions, go to office hours, write emails. Most importantly, don't get stuck and do nothing about it. Take your education into your own hands. Don't be like the people on the broken escalator.
College has changed a lot since I was last here. Sure we had laptops and cell phones, but for the most part, students dutifully took notes on paper. I kept all of my college notebooks, which I actually used a few when teaching. But now, everyone seems to download the powerpoint onto their MacBook Pro, open it when the professor starts and proceed to Facebook or Amazon. I am shocked by the number of people that don't really pay attention during pharmacy school. Then they complain about having to rewatch the lectures and not doing as well on their exams.
I found success this semester with a very simple set up. I download the PPT file and convert it into a PDF of two slides per page. I upload it to the Dropbox to transfer to my iPad and open in NoteTakerHD. That is were I take my notes. Most importantly, since the iPad only does one thing at a time, I can't lose myself in other websites. I also read the books, make study guides, based on the objectives listed by the professor, and make flash cards on Quizlet.
My problem is to remember that education is more than making A's in the classroom. As introverted as I am, I must force myself to get out there and participate in the various clubs and talk to professors. They gave us a professor as a mentor, but I failed to utilize him. I am going to correct that next year. I did some CAPS activities, but I plan to do much more this year. I am now the webmaster/historian, putting me into a leadership position. I am joining the Recruitment Ambassadors to spread to word about pharmacy and specifically the UNC Eshelman School of Pharmacy. I plan to join the SHAC clinic and actively work with local patients during the semester. Take control of your education and make your weaknesses you strengths.
College has changed a lot since I was last here. Sure we had laptops and cell phones, but for the most part, students dutifully took notes on paper. I kept all of my college notebooks, which I actually used a few when teaching. But now, everyone seems to download the powerpoint onto their MacBook Pro, open it when the professor starts and proceed to Facebook or Amazon. I am shocked by the number of people that don't really pay attention during pharmacy school. Then they complain about having to rewatch the lectures and not doing as well on their exams.
I found success this semester with a very simple set up. I download the PPT file and convert it into a PDF of two slides per page. I upload it to the Dropbox to transfer to my iPad and open in NoteTakerHD. That is were I take my notes. Most importantly, since the iPad only does one thing at a time, I can't lose myself in other websites. I also read the books, make study guides, based on the objectives listed by the professor, and make flash cards on Quizlet.
My problem is to remember that education is more than making A's in the classroom. As introverted as I am, I must force myself to get out there and participate in the various clubs and talk to professors. They gave us a professor as a mentor, but I failed to utilize him. I am going to correct that next year. I did some CAPS activities, but I plan to do much more this year. I am now the webmaster/historian, putting me into a leadership position. I am joining the Recruitment Ambassadors to spread to word about pharmacy and specifically the UNC Eshelman School of Pharmacy. I plan to join the SHAC clinic and actively work with local patients during the semester. Take control of your education and make your weaknesses you strengths.
Wednesday, July 9, 2014
IPPE Yippies
 During the entire month of May, I interned at the University of North Carolina Hospital. The coveted Chapel Hill placement gave me a ton of opportunities that other PY1s may not have experienced. The first thing you need to know is that UNC Health Care is huge. The campus covers the entirety of South Campus and houses the Memorial Hospital, Children's Hospital, Women's Hospital, Neurosciences and Cancer Center. There are three amazing places to eat and the world's largest Starbucks (24/7 and a 20% discount).
During the entire month of May, I interned at the University of North Carolina Hospital. The coveted Chapel Hill placement gave me a ton of opportunities that other PY1s may not have experienced. The first thing you need to know is that UNC Health Care is huge. The campus covers the entirety of South Campus and houses the Memorial Hospital, Children's Hospital, Women's Hospital, Neurosciences and Cancer Center. There are three amazing places to eat and the world's largest Starbucks (24/7 and a 20% discount). My internship was called the Introductory Pharmacy Practice Experience (IPPE). Working with a preceptor, we are expected to learn the ins and outs of being a hospital pharmacist. Almost every other pharmacy school sends their first year students into the community first, but we do things a bit differently. You definitely start off feeling out of place on a content level and lost on a physical level. My goal at the beginning was simple - find out if there was any area of hospital pharmacy that I could not see myself doing. In the end, I felt comfortable throughout and could not find anything to mark off the list of possible future careers.
I and my 14 fellow IPPEs experienced many different areas of hospital pharmacy during our rotation in May. I feel that we probably received a broader education than IPPEs that went off to other hospitals, especially the smaller ones. While spending more than one day in an area would give depth to the experience, I would not trade the breadth. I will be writing about each of the different areas that we went in much more detail throughout the month. I have a lot to say about each of them and maybe they help some other people.
One major difference to mention now would be the set up. Instead of a single pharmacist in charge of us, UNC delegates the IPPE education to two outgoing PGY2-Administration residents. The Pharmacy Administration Residency is a two year program and they do a lot regarding management and leadership. As a former coach, I have great respect for those particular aspects of the pharmacy world. Our 15 students were divided into two groups for a challenge to have a pizza lunch with the Director of Pharmacy at the hospital. My team, the IPPE Yippies, took on the Conformational Floppies through several tasks.
- We wrote on Wiki site through the School of Pharmacy about pretty much anything. Whoever wrote the most received the most points for their team. I hadn't planned on doing, but a another student pounced on it early. I soon made my goal to catch her, but she had such a huge lead that I could only achieve second place.
- One day we debated the merits of the 340B program that UNC Hospitals use for cheaper medications. Our team won that by having the pro-340B side with all of the judges being hospital pharmacy residents. I will write more about 340B later.
- We wrote SBAR memos to the director to make suggestions about improving the hospital. SBAR is a common method of communication in the hospital to deliver ideas or information quickly and efficiently. The Conformational Floppies dominated us in this one. They wrote 7 suggestions while my team only wrote 3 (and I had 2 of them). At this point, it did not seem like my team was interested in winning the competition.
- Finally, we mapped out the flow of medication through the hospital from order, verification, dispensation and administration. Each team had to make one in a group effort to understand the hospital. The Conformational Floppies apparently met for several hours on a Sunday to do theirs. The IPPE Yippies put it off until the last second. I tried to organize a lunch meeting to work on it, but it was a no go. We really did not want to win apparently. On the last day, we knew that we had to turn something in, so someone put it together quickly. We looked it over on Google Docs and submitted it with no color and very little effort. Whichever team won the map would win for the month.
Tuesday, July 8, 2014
TED Talk Tuesday: Adam Savage
 The Mythbusters bring a excitement and beauty to the scientific process that inspires millions of kids in the science classroom. I used the Mythbusters a lot during my teaching days to help them understand the scientific method. Especially in Physical Science, we would watch an episode after every test and they would dutifully require the Hypothesis (Myth), Experiment, Data, and Conclusion (Busted/Confirmed/Plausible). Kids need to learn that "Failure is always an option". Too many people see failure and quit, but the Mythbusters rightfully view failure as an opportunity to try again.
The Mythbusters bring a excitement and beauty to the scientific process that inspires millions of kids in the science classroom. I used the Mythbusters a lot during my teaching days to help them understand the scientific method. Especially in Physical Science, we would watch an episode after every test and they would dutifully require the Hypothesis (Myth), Experiment, Data, and Conclusion (Busted/Confirmed/Plausible). Kids need to learn that "Failure is always an option". Too many people see failure and quit, but the Mythbusters rightfully view failure as an opportunity to try again.
Adam Savage brings some of that wonder to the TED stage in this TED Ed Talk about how simple ideas lead to important scientific discoveries such as the speed of light or the circumference of the Earth. We are all explorers attempting to understand the world before us. Somethings are known, but a lot remains in question. As the Mythbusters show, some of the things we know are not.
The best part about these TED Ed talks is that it is animated. My students always liked the animated talks more than normal lectures. They can follow the images even when they don't fully understand the words being said. So if you are showing TED Talks in classes, I urge you to check out their animated videos.
Enjoy!
Monday, July 7, 2014
Hobby Lobby and the Supreme Court Misjudge Emergency Contraceptives
This past week, the US Supreme Court decided that "closely held" companies can opt out of covering particular forms of birth control for their employee insurance based on a "sincere" religious objection. The sincerely-religious owners of Hobby Lobby objected to the Obamacare requirement of insurance plans to cover birth control for their employees. To be fair, they did not object to all forms of birth control, just the ones that they felt were the same as causing abortions. Unfortunately, many people continue to believe that the morning after pill, emergency contraceptive, Plan B, or levonorgestrel is an abortion-causing pill. The ruling also applied to Inter-Uterine Devices (IUDs) for the same reason.
One problem - these pills do not cause abortions. An abortion refers to the medical termination of a pregnancy. Levonorgestrel and IUDs prevent a pregnancy from occurring in the first place. Thus preventing the potential for an employee to seek an abortion due to an unwanted pregnancy. Hobby Lobby, and the other conservative companies that will soon be refusing to pay of emergency contraceptives, do provide health insurance plans that cover most of the other forms of oral contraception. Normal contraceptives must be taken daily and generally at the same time everyday. Missing a dose can prevent the hormonal control "the pill" is attempting to maintain. This is were Plan B comes in. If a woman forgets to take her normal birth control pill, levonorgestrel can help. And a lot of people forget to take their pills.
 So how does Plan B work? Levonorgestrel is a synthetic version of progestin. Progestin prevents ovulation. Pregnancy actually only occurs during a very small window of about 4 or 5 days, sort of. The sperm can survive for a while waiting for an egg to be released, but the egg lasts for less than a day. Oral contraceptives prevent the release on an egg over the course of the month. An emergency contraceptive like levonorgestrel serves as a surge of progestin than prevents ovulation about 72 hours. To work best, Plan B should be taken as soon as possible after unprotected sex, but it doesn't always work. Levonorgestrel does not work after ovulation. So if the egg is out, pregnancy is possible whether you take the pill or not. If fertilization has already occurred, levonorgestrel will not help either. Some thought that it could prevent implantation of a fertilized egg, but no evidence supports that mechanism of action. And one thing that it definitely does not do is terminate a pregnancy.
So how does Plan B work? Levonorgestrel is a synthetic version of progestin. Progestin prevents ovulation. Pregnancy actually only occurs during a very small window of about 4 or 5 days, sort of. The sperm can survive for a while waiting for an egg to be released, but the egg lasts for less than a day. Oral contraceptives prevent the release on an egg over the course of the month. An emergency contraceptive like levonorgestrel serves as a surge of progestin than prevents ovulation about 72 hours. To work best, Plan B should be taken as soon as possible after unprotected sex, but it doesn't always work. Levonorgestrel does not work after ovulation. So if the egg is out, pregnancy is possible whether you take the pill or not. If fertilization has already occurred, levonorgestrel will not help either. Some thought that it could prevent implantation of a fertilized egg, but no evidence supports that mechanism of action. And one thing that it definitely does not do is terminate a pregnancy.
So here's where I am concerned about the Hobby Lobby ruling. Forcing employers to cover abortions is controversial, so I am okay with taking that out as a compromise. But allowing them to object to certain forms of birth control because they believe that they cause an abortion is wrong. Plan B does not cause abortions (period). We study the mechanism of action. We know how it works. It prevents pregnancy. This is not about a belief system. This is an education problem. They can believe that it causes an abortion, but they are flat out wrong.
One problem - these pills do not cause abortions. An abortion refers to the medical termination of a pregnancy. Levonorgestrel and IUDs prevent a pregnancy from occurring in the first place. Thus preventing the potential for an employee to seek an abortion due to an unwanted pregnancy. Hobby Lobby, and the other conservative companies that will soon be refusing to pay of emergency contraceptives, do provide health insurance plans that cover most of the other forms of oral contraception. Normal contraceptives must be taken daily and generally at the same time everyday. Missing a dose can prevent the hormonal control "the pill" is attempting to maintain. This is were Plan B comes in. If a woman forgets to take her normal birth control pill, levonorgestrel can help. And a lot of people forget to take their pills.
So how does Plan B work? Levonorgestrel is a synthetic version of progestin. Progestin prevents ovulation. Pregnancy actually only occurs during a very small window of about 4 or 5 days, sort of. The sperm can survive for a while waiting for an egg to be released, but the egg lasts for less than a day. Oral contraceptives prevent the release on an egg over the course of the month. An emergency contraceptive like levonorgestrel serves as a surge of progestin than prevents ovulation about 72 hours. To work best, Plan B should be taken as soon as possible after unprotected sex, but it doesn't always work. Levonorgestrel does not work after ovulation. So if the egg is out, pregnancy is possible whether you take the pill or not. If fertilization has already occurred, levonorgestrel will not help either. Some thought that it could prevent implantation of a fertilized egg, but no evidence supports that mechanism of action. And one thing that it definitely does not do is terminate a pregnancy.So here's where I am concerned about the Hobby Lobby ruling. Forcing employers to cover abortions is controversial, so I am okay with taking that out as a compromise. But allowing them to object to certain forms of birth control because they believe that they cause an abortion is wrong. Plan B does not cause abortions (period). We study the mechanism of action. We know how it works. It prevents pregnancy. This is not about a belief system. This is an education problem. They can believe that it causes an abortion, but they are flat out wrong.
Friday, July 4, 2014
John Oliver Takes Down Dr. Oz
Corespondent John Oliver left the Daily Show for his own show on HBO called Last Week Tonight. On the episode from June 22nd, Oliver went after Dr. Oz who had appeared before Congress the previous week. Dr. Oz has made a ton of money teaching people to be healthy. He wrote You - The Owners Manuel and has a daily television show. On that show he often promotes products to help you lose weight. More recently, Oz hawked Green Coffee Extract to shed pounds describing the product a a magic cure. Under oath, Oz admitted that there is no such thing as a magic cure, despite his use of the phrase over and over again.
The real problem is nutritional supplements that suggest they offer cures for numerous maladies. Dr. Oz got caught filling time with hype and taking money from a $32-billion business. FDA has very little control over nutritional supplements despite their label as "food". Some products are no better than placebos and some cause health problems rather than cure them. When the FDA sought to establish control over the market, the supplement lobby responded to squashed such laws by scaring the public and buying congressmen.
John Oliver details the long story of fake cures and FDA oversight in this excellent commentary. It goes a little off the rails at the end, but he is a comedian. Enjoy.
The real problem is nutritional supplements that suggest they offer cures for numerous maladies. Dr. Oz got caught filling time with hype and taking money from a $32-billion business. FDA has very little control over nutritional supplements despite their label as "food". Some products are no better than placebos and some cause health problems rather than cure them. When the FDA sought to establish control over the market, the supplement lobby responded to squashed such laws by scaring the public and buying congressmen.
John Oliver details the long story of fake cures and FDA oversight in this excellent commentary. It goes a little off the rails at the end, but he is a comedian. Enjoy.
Thursday, July 3, 2014
PY1 Review - Pharmaceutical Care Lab
The Pharmaceutical Care Lab (PCL) course was the only interactive class of our first year. Once a week, we would spend half the day in the lab working on a variety of topics. Instead of sitting in a stale classroom, we worked in small groups through assignments, discussions, check-offs, and compounding. I enjoyed the variety of the courses.
The most stressful part of PCL was the Top 200 Drug List. Each week we had a new list of 8-10 drugs to memorize the Generic Name, Brand Name, Therapeutic Class, and Common Indication. The weekly quiz wasn't too bad, but you did have to spell everything exactly. The Staying on Track Quiz brought about 4 weeks of drugs together and the final exam from each semester put 100 drugs into a single test. I quickly found that Quizlet offered the best method to study the drug names with rapid repetition that required correct spelling. You could study on your computer and on your phone as you rode the bus to class. For anyone that has to memorize anything, I suggest Quizlet. Below I include the Top 200 Drugs we had to learn this year. During PY2, we will use the same drugs but add much more detail including doses, side effects, and precautions.
 During each semester, we produced 4 compounded prescriptions. Sometimes a patient requires medication that is not commercially available or in a different form. Pharmacists are licensed to compound products. Some students loved compounding but others hated it. To me, it was just like any chemistry class. I liked the part. We made Benadryl solutions, Ketoprofen creams, nasal sprays, and much more. The most interesting to me was a menthol troche to soothe irritated throats. In addition to preparing the compounded drugs, we had to counsel the patient on how to use the product. I suspect more people we worried about counseling that preparation. For each product, you explained the way to take the medication, what to watch out for, and some other parts. In the profession, pharmacists can do from zero to all compounding. In the special formulations area of the hospital, compounding happens all the time. Some pharmacies do nothing but compound products for local hospitals and patients (but some got in trouble for doing too much the wrong way - there will be a post about that later). Then again, some pharmacists will never compound a products. But all pharmacists have to counsel patients on medications.
During each semester, we produced 4 compounded prescriptions. Sometimes a patient requires medication that is not commercially available or in a different form. Pharmacists are licensed to compound products. Some students loved compounding but others hated it. To me, it was just like any chemistry class. I liked the part. We made Benadryl solutions, Ketoprofen creams, nasal sprays, and much more. The most interesting to me was a menthol troche to soothe irritated throats. In addition to preparing the compounded drugs, we had to counsel the patient on how to use the product. I suspect more people we worried about counseling that preparation. For each product, you explained the way to take the medication, what to watch out for, and some other parts. In the profession, pharmacists can do from zero to all compounding. In the special formulations area of the hospital, compounding happens all the time. Some pharmacies do nothing but compound products for local hospitals and patients (but some got in trouble for doing too much the wrong way - there will be a post about that later). Then again, some pharmacists will never compound a products. But all pharmacists have to counsel patients on medications.
We began learning about Medication Therapy Management by looking a patient's med lists and searching for duplications and interactions. We took vital signs, including blood pressure. We interviewed a patient. We practiced and passed aseptic technique. The PCL covers a lot of ground. It also lets PY3s work as Teaching Assistants for the PY1s. I am looking forward to what we will do next year.
The most stressful part of PCL was the Top 200 Drug List. Each week we had a new list of 8-10 drugs to memorize the Generic Name, Brand Name, Therapeutic Class, and Common Indication. The weekly quiz wasn't too bad, but you did have to spell everything exactly. The Staying on Track Quiz brought about 4 weeks of drugs together and the final exam from each semester put 100 drugs into a single test. I quickly found that Quizlet offered the best method to study the drug names with rapid repetition that required correct spelling. You could study on your computer and on your phone as you rode the bus to class. For anyone that has to memorize anything, I suggest Quizlet. Below I include the Top 200 Drugs we had to learn this year. During PY2, we will use the same drugs but add much more detail including doses, side effects, and precautions.
During each semester, we produced 4 compounded prescriptions. Sometimes a patient requires medication that is not commercially available or in a different form. Pharmacists are licensed to compound products. Some students loved compounding but others hated it. To me, it was just like any chemistry class. I liked the part. We made Benadryl solutions, Ketoprofen creams, nasal sprays, and much more. The most interesting to me was a menthol troche to soothe irritated throats. In addition to preparing the compounded drugs, we had to counsel the patient on how to use the product. I suspect more people we worried about counseling that preparation. For each product, you explained the way to take the medication, what to watch out for, and some other parts. In the profession, pharmacists can do from zero to all compounding. In the special formulations area of the hospital, compounding happens all the time. Some pharmacies do nothing but compound products for local hospitals and patients (but some got in trouble for doing too much the wrong way - there will be a post about that later). Then again, some pharmacists will never compound a products. But all pharmacists have to counsel patients on medications. We began learning about Medication Therapy Management by looking a patient's med lists and searching for duplications and interactions. We took vital signs, including blood pressure. We interviewed a patient. We practiced and passed aseptic technique. The PCL covers a lot of ground. It also lets PY3s work as Teaching Assistants for the PY1s. I am looking forward to what we will do next year.
Wednesday, July 2, 2014
Self-Care - Vitamin C
In first semester lab, each group of 3-4 students delivered a 20 minute presentation on an herbal remedy. Self-care refers to the items that customers by at the front of the store and routinely forget to inform their doctors and pharmacists about. Herbal supplements are big business making huge profits as a trendy alternative to a prescription without the risky part of actually testing the product through clinical trials. Labeled as dietary supplements, herbals do not have to actually provide data about whether or not the product works. Then again, they cannot say that the product does work either. A lot of these products rely on anecdotal evidence and the mythos of ancient, traditional or alternative medicine.
To be fair some of the products worked. A little. Most were inconclusive. And one big one - St. John's Wort - interacts with almost every pharmaceutical drug out there and can be dangerous in combinations. My group's topic was no different. We had Vitamin C.
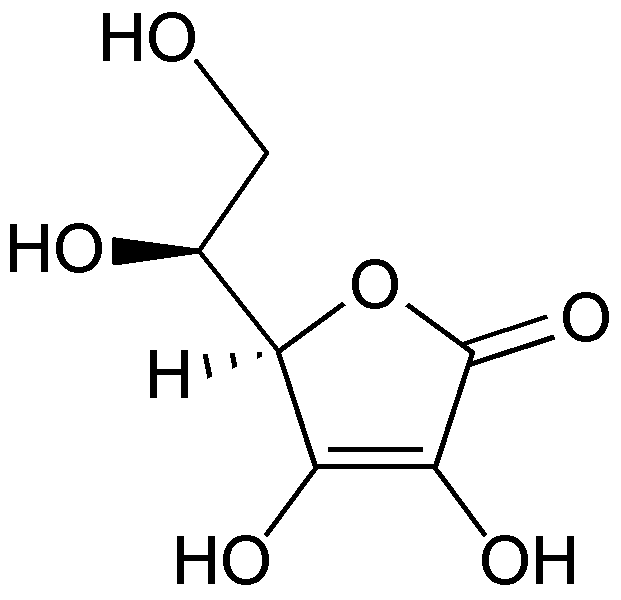 |
| Molecular structure of Vitamin C (ascorbic acid) |
Vitamin C, you know, occurs naturally in citrus fruits. Our body needs it and a lack of the vitamin results in Scurvy. Sailors and pirates would return from see emaciated and losing their teeth. It was determined that they lacked Vitamin C and prescribed oranges, lemons and limes. Vitamin C works great as a treatment for scurvy. But the makers of EmergenC are targeting sailors. Rather, they trick people into thinking that large amounts of Vitamin C could prevent the common cold. They even had a two-time Nobel laureate on their side. Linus Pauling loved Vitamin C taking over a 1000 mg a day or about 1667% greater than the recommended allowance. He claimed it kept him from getting sick, even when he obviously suffered from a cold. Later he claimed that it prevented cancer, even though he and his wife both died of cancer. In short the Pauling promotion of Vitamin C lingers into confusion today. Despite the assertions of the eminent scientist, no evidence ever supported him.
In our group, I landed the introductory role. My job was to get everything started and get people interested. I only presented the first five slides, but I researched and wrote one of the slides at the end (about the Cochrane Review). While I am posting this on here, I do not want to take credit on the interwebs for the entire project. Vitamin C deeply interested me and I enjoyed the history of this great confusion. My group did a great job and they should receive the credit they deserve.
Tuesday, July 1, 2014
TED Talk Tuesday - Apollo Robbins
I love magic. The acting, the misdirection. All of it playing on the frailty of our senses and perceptions. Magic and neuroscience go together. Apollo Robbins is a magician on the show Brain Games. He came to TED to talk about the art of misdirection. People are not as perceptive as they believe themselves to be. A little feint in one direction distracts us from the real action the other way. Magicians master this skill and teach us a lot about our ability to perceive the world around us.
Monday, June 30, 2014
PY1 Review - Pharmacotherapy
Pharmacotherapy produced divergent opinions. Some really hated the class, but other really enjoyed it. I was on the positive side and appreciated the curveballs thrown by the professor. Each semester for the remainder of the classroom portion of the PharmD program will have a therapy component. This course takes a common disorder and focuses on the way we treat it. It can't get anymore straight forward. This is the purpose of any health career, so pharmacotherapy is perhaps the most prescient class of our program (up there with PCL).
The second semester of the PY1 focuses on the #1 reason a patient encounters a health care provider - PAIN. Pain lets us know that something is wrong with our body and sends the patient to see the doctor. Everyone takes some kind of pain medicine, whether Advil and Tylenol up to Percocet and Morphine. Our task this past spring was to understand pain management.
We started by learning about medical records. Some people didn't seem to understand why. While, we do not perform the physical examination or run the clinical labs, we do have to understand what is in the file. Is the patient's potassium too high or too low? Does the positive stool guaiac have any relevance to the patient's abdominal pain? We have to be able to distinguish the pertinent positives of a medical history from pertinent negatives. This was perhaps the most confusing part to the majority of the class. I hope that my understanding can work for you. A pertinent positive refers to any abnormality in a patient's chart. If a value is outside the normal range, it is important to note. A pertinent negative refers to something that we would expect to be wrong, but is okay. So if you hypothesize that the patient has internal bleeding, but a high hematocrit that would be a pertinent negative as bleeding should decrease your blood count. Reading an understanding a chart helps the doctor diagnose a disorder, but it helps the pharmacist manage the appropriate therapy and prevent potential errors.
 Finally, we moved onto the topic of pain. We talked about metastatic pain from cancer and the various forms of joint pain from arthritis. Choosing the appropriate pain medicine depends on severity and side effects. Opioids are the best at reducing pain, but also suppress breathing. Surgical patients blow hard into a spirometer every hour to clear their lungs of potential bacteria as the morphine keeps them from doing so on their own. Patients with severe pain take a standing dose of an opioid but also need a rescue dose for breakthrough pain. The pharmacist must check the doses, convert between one opioid to the next and watch for side effects.
Finally, we moved onto the topic of pain. We talked about metastatic pain from cancer and the various forms of joint pain from arthritis. Choosing the appropriate pain medicine depends on severity and side effects. Opioids are the best at reducing pain, but also suppress breathing. Surgical patients blow hard into a spirometer every hour to clear their lungs of potential bacteria as the morphine keeps them from doing so on their own. Patients with severe pain take a standing dose of an opioid but also need a rescue dose for breakthrough pain. The pharmacist must check the doses, convert between one opioid to the next and watch for side effects.
 In the case of arthritis, pain medicines must also be used with other therapies. Also start with the lowest possible solution - Tylenol and exercise. Maybe braces could be required to stabilize the joints, but if the problem progresses, move up to NSAIDs like Advil. Unfortunately, NSAIDs cause a lot of problems like gastrointestinal bleeding, kidney problems, and clotting issues. Millions of people take NSAIDs everyday without recognizing the possible consequences. Most people take them for acute reasons like a sprain or headache, but chronic use can be a problem like with arthritis. Whether osteoarthritis, rheumatoid arthritis or gout, the disorder will affect them for the rest of their lives. Now you need treatments like allopurinol to lower the uric acid in the patient's blood to prevent gout flares. Or methotrexate or Remicade to fight the debilitation of rheumatoid arthritis. Pain can be quite complicated and the medications can cause their own problems.
In the case of arthritis, pain medicines must also be used with other therapies. Also start with the lowest possible solution - Tylenol and exercise. Maybe braces could be required to stabilize the joints, but if the problem progresses, move up to NSAIDs like Advil. Unfortunately, NSAIDs cause a lot of problems like gastrointestinal bleeding, kidney problems, and clotting issues. Millions of people take NSAIDs everyday without recognizing the possible consequences. Most people take them for acute reasons like a sprain or headache, but chronic use can be a problem like with arthritis. Whether osteoarthritis, rheumatoid arthritis or gout, the disorder will affect them for the rest of their lives. Now you need treatments like allopurinol to lower the uric acid in the patient's blood to prevent gout flares. Or methotrexate or Remicade to fight the debilitation of rheumatoid arthritis. Pain can be quite complicated and the medications can cause their own problems.
The second semester of the PY1 focuses on the #1 reason a patient encounters a health care provider - PAIN. Pain lets us know that something is wrong with our body and sends the patient to see the doctor. Everyone takes some kind of pain medicine, whether Advil and Tylenol up to Percocet and Morphine. Our task this past spring was to understand pain management.
We started by learning about medical records. Some people didn't seem to understand why. While, we do not perform the physical examination or run the clinical labs, we do have to understand what is in the file. Is the patient's potassium too high or too low? Does the positive stool guaiac have any relevance to the patient's abdominal pain? We have to be able to distinguish the pertinent positives of a medical history from pertinent negatives. This was perhaps the most confusing part to the majority of the class. I hope that my understanding can work for you. A pertinent positive refers to any abnormality in a patient's chart. If a value is outside the normal range, it is important to note. A pertinent negative refers to something that we would expect to be wrong, but is okay. So if you hypothesize that the patient has internal bleeding, but a high hematocrit that would be a pertinent negative as bleeding should decrease your blood count. Reading an understanding a chart helps the doctor diagnose a disorder, but it helps the pharmacist manage the appropriate therapy and prevent potential errors.
Subscribe to:
Posts (Atom)